773
Views & Citations10
Likes & Shares
The scourge viral
hepatitis is life threatening and is about to become an epidemic particularly
in Aliero metropolis. This study tries to survey the prevalence of hepatitis B
and C viruses in Aliero metropolis from 2011 to 2015. This was done by scientifically
and systematically gathering data from the hospital laboratory records.
Furthermore, surveys were conducted from human subjects; after collecting an
ethical clearance from the state ministry of health, informed consents and assents were all sought for from
eligible participants respectively (1-65 years) then blood samples were drawn
from volunteers for screening against HBV and HCV respectively according to
protocol: commercial kits were used, according to the manufacturer's
instructions (Abbott Laboratories, Abbott Park, IL), to detect hepatitis B
surface antigen (HBsAg; AUSZYME monoclonal EIA) and hepatitis C virus (HCV).
The Blood samples collected after informed consent and assent from volunteers
were evaluated for the presence and qualitative determination of HBV and HCV
surface antigens. The maximum line on the strip would be observed; the strip
will be placed on a non-absorbent surface. The strip will be set for 15 min,
awaiting the red line to appear or not. Two distinct red lines, one on the control
(C) region while other on the test (T) region. The intensity of the red color
on the test line varies depending on the concentration of the HBsAg and HCV in
the specimen. Therefore shade of red line in (T) region will be considered
positive while on the control (C) region and no shade of red color on the test
(T) region it as negative. The result of this work along with the existing data
which was given to us as additional information from the hospital staff
suggests that the prevalence of hepatitis B virus and hepatitis C virus is year
dependently increasing.
INTRODUCTION
Approximately
350 million people are infected with HBV worldwide and the World Health
Organization (WHO) estimates that approximately 170 million people are infected
with HCV. HBV and HCV infection account for a substantial proportion of liver
diseases worldwide. Because the two hepatotropic viruses share same modes of
transmission, co-infection with the two viruses is not uncommon, especially in
areas with a high prevalence of HBV infection and among people at high risk for
parenteral infection. The exact number of patients infected with both HCV and
HBV is unknown. Hepatitis is simply an inflammation of the liver; it may be
caused by exposure to certain chemicals, autoimmune diseases or by bacterial
infections but is often caused by one of several viruses [1,2]. The Hepatitis
virus lives in the blood and other body fluids and is transmitted from one
person to person through unprotected sexual intercourse with an infected person,
sharing infected needles or other sharp agents that break the skin [1]. Hepatitis
is a serious health concern worldwide. Countries with the greatest prevalence
include Africa, South America, eastern European countries and Asian countries.
Incidence and mortality rates vary with each type of the disease: Being an
inflammatory disorder of the liver that may be caused by viruses, drugs and
toxins, etc., symptoms include jaundice (yellowing of skin and eyes) and
fever-like symptoms. The three major viruses that affect the liver, hepatitis
A, B and C (HAV, HBV and HCV) differ according to mode of transmission,
pathology and prognosis. Generally, the viruses are transmitted through feces,
blood or bodily fluid that contains blood. Fecal contamination of water and food,
eating undercooked shellfish and using contaminated intravenous drug needles
are all common routes of transmission. Toxins like alcohol and anti-HIV drugs
can lead to non-viral hepatitis.
Hepatitis is considered a sexually transmitted
disease (STD) because
it can be contracted and spread through intercourse, contact with genitals and
the anus, semen, vaginal fluids and saliva. It is over 100 times more
infectious than HIV. Certain high-risk sexual behaviors have led to an
increased prevalence of hepatitis in men who have sex with men (MSM).
HBV
is a major cause of liver disease morbidity and mortality worldwide, accounting
for over 360 million cases of chronic hepatitis and 620,000 deaths per a year
[3]. It is hyper endemic (i.e., >8% of the population infected) in
Sub-Sahara Africa (SSA) and a major cause of chronic liver disease [4-6], Perz
et al. [7] estimated that 44% of cirrhotic liver disease and 47% of hepatocellular
carcinoma cases in SSA are attributed to HBV [8]. A highly effective and
inexpensive recombinant DNA vaccine for hepatitis B has been available since
1982 and debuted in Nigeria in 1995. Unfortunately, vaccination programs in
Nigeria have not received adequate attention or funding by the government.
Further, community misconceptions have hindered increasing coverage rates
[9,10]. The United Nations Children's Fund (UNICEF) and the World Health
Organization (WHO) estimated that only 41% of Nigerians were vaccinated against
HBV in 2013 [11]. The risk of contracting HBV in Nigeria is substantial, not
only due to low vaccination rates but also given that as many as 75% of the
population will be exposed [12]. Investigators have reported varying national
and risk group-specific estimates. Prior reports suggest a prevalence of 10-15%
in the average risk Nigerian population [13]. In Nigeria, investigators have
found high HBV prevalence among surgeons (25.7%) [14], voluntary blood donors
(23.4%) [15] and infants (16.3%) [16]. A 2012 study in Kano Nigeria found that
among 440 HIV positive patients, 12.3% were co-positive for HBV [17]. Although,
pregnant women are generally considered low risk for HBV infection, rates as
high as 11% have been reported in Nigeria [18]. Hepatitis B is the commonest
cause of chronic liver disease in Nigeria. In southern parts of the country, up
to 58.1% of patients with chronic liver disease were found HBsAg positive [14].
Several authors report on the prevalence of HBV among sub-populations in
Nigeria with estimates varying depending on population studied and methods
used. However, there is no reliable national survey of HBV exposure in the
average risk population and in subgroups most likely to benefit from early
detection, surveillance, and treatment.
AIM
The
aim of this work is to establish the prevalence of hepatitis B virus and also
hepatitis C virus in Aliero metropolis.
The
objectives are:
(i)
To collect
systematic and scientific data already gathered and documented by the hospital
staff of the General hospital of people who have been tested positive for HBV
and HCV.
(ii)
To draw blood
from volunteer patients after their consent/assent is well sought for and
screen the blood for the presence of HBV and HCV, respectively.
Justification for the study
Justification
for this work is based on the fact that, many women who come for Antenatal
care, child birth and blood donors both men and women in this health facility
(New General Hospital Aliero) were found to be positive for either HBV or HCV
or even both and continued to live with the disease in ignorance hence the need
for the study.
MATERIALS AND METHOD
Sample collection
Data
from the laboratories and card records office of the General Hospital Aliero
were gathered for the purpose of this work. Additionally, after informed
consent/assent was sought samples of blood were collected from human subjects
(male and female of 1 to 65 years old) who often come to the General Hospital
Aliero, using 5 ml syringes and transfer in to test tubes containing 2 to 3 drops
of anticoagulant and spun for 2 to 3 min using centrifuge machine and plasma
was obtained which was used to determine both HBsAg and HCV, respectively.
Serologie testing
Commercial
kits were used, according to the manufacturer's instructions (Abbott Laboratories,
Abbott Park, IL), to detect hepatitis B surface antigen (HBsAg; AUSZYME
monoclonal EIA), anti-HBsAg antibodies (AUSAB), and hepatitis C virus (HCV)
antibodies (HCV EIA 2.0). Sera positive for HCV antibodies by EIA were tested
by use of the RIBA HCV 2.0 strip immunoblot assay (Chiron, Emeryville, CA).
Determination of HBV and HCV
RESULTS
DISCUSSION
Dual
infection with HBV and HCV is not uncommon just as reported by Liu and Hou [19]
that particularly in geographic areas where a high endemic level of both
infections is documented, such as Southeast-Asia and Mediterranean. In general,
the prevalence is around 10-20% in patients with chronic HBV infection and
2-10% of anti-HCV-positive patients to have markers of HBV infection. Aliero is
one of the local Government headquarters in Kebbi State, North-Western Nigeria,
Africa, with a population of hundreds of thousands of people and is a
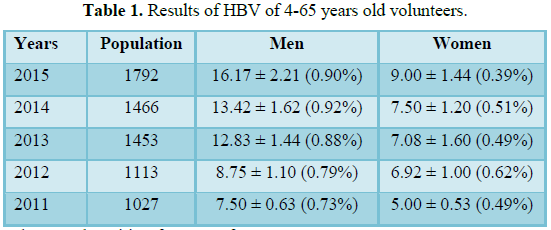
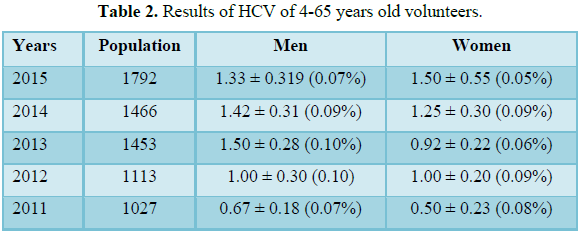
commercial center due to its high onions cultivation. The results of this study
shows that men appear to be more predisposed to the susceptibility of both
hepatitis B virus as well as the hepatitis C virus. All the more, there appears
to be a gradual but steady increase in the incidence rate of the infections
year dependently for both HBV and that of HCV, respectively. This might likely
be due to unawareness of the community and its environment and hence no
regulatory measures to reduce or control the incidence or possibly due to the
same reason of unawareness plus cultural practices which encourage
intra-marriages (very common) and therefore, spreading the disease unawares
among family members. The prevalence of hepatitis B and C among the men might
not suggest a greater incidence/endemicity as polygamy is the order of the day
in the metropolis, which will eventually bridge the gap or even exceed as the
case may be. The year 2011 and 2013 which appears to have low incidence might
actually represent a true picture or not of the incidence/endemicity this due
to the fact that some people only come to health facilities when they fall sick
particularly in the rainy seasons when malaria incidence is usually high.
Another reason for the steady gradual increase of the infection is probably due
to one Government School of Health Technology Jega, Kebbi State Nigeria meant
to improve on the lives of the community health wise; ignorantly people involve
into administrations of drugs using one syringe and needle for a whole people
in the family per time when sick (personal communications) and even worst blood
draws and blood transfusions are being done without proper blood check and
cross matching before the transfusion (which is usually obtained in the health
facilities) on the assumptions that these people are the same health workers
you meet in the health facilities and also that they will reduce cost of
transporting themselves as well purchase of cards and other items in the
hospitals.
CONCLUSION/RECOMMENDATION
Understanding
the community-specific epidemiology of disease, which may vary greatly among
other communities, is crucial for identifying the most appropriate preventive
and control measures. An overview of the local epidemiology of viral hepatitis
in Aliero metropolis is given in this paper. The overall prevalence of
hepatitis B and C in the community cannot be reported as low despite the so
called low values because only a small fraction were actually sampled in the
general population of the community due to so many limitations/factors, because
so many people are carrying the disease ignorantly. It is reported that
Hepatitis B incidence and prevalence began to decline significantly following
the introduction of universal hepatitis B vaccination in 1999 in Croatia.
Information on HBsAg seroprevalence is derived from routine testing of certain
subpopulations (pregnant women, blood donors) and seroprevalence studies mostly
targeted at high-risk populations. Universal childhood vaccination against
hepatitis B remains the main preventive measure. Similarly, we recommend a
general mobilization for people to know their status, testing for immunity one
to two months after the third dose of hepatitis B vaccine for children,
health-care workers and general population of the community. We also recommend
a major preventive measure, i.e., ensuring safety of blood
products/transfusions, prevention of drug misuse/abuse.
1.
Redmond WA (2008) Liver. Microsoft Student [DVD]
Microsoft Corporation.
2.
Ahmedin J, Taylor M, Ram CT, Asma G, Alicia S, et al.
(2010) New section in cancer offering timely and targeted information. Cancer J
Clin 54.
3.
Centers for Disease Control and Prevention (1997)
Summary of notifiable diseases, United States. MMWR Morb Mortal Wkly Rep 46:
1-88.
4.
Hadler SC, Erben JJ, Francis DP, Webster HM, Maynard JE
(1982) Risk factors for hepatitis A in day-care centers. J Infect Dis 145:
255-256.
5.
Koff RS (1995) Seroepidemiology of hepatitis A in the
United States. J Infect Dis 171: 19-23.
6.
Metropolitan
Health District (1997) Health and demographic statistics: Selected notifiable
communicable diseases. http://iweb.ci.sat.tx.us/health/Profiles/Comm_l2.htm
7.
Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP
(2006) The contributions of hepatitis B virus and hepatitis C virus infections
to cirrhosis and primary liver cancer worldwide. J Hepatol 45: 529-538.
8.
McQuillan GM, Townsend TR, Fields HA, Carroll M, Leahy
M, et al. (1989) Seroepidemiology of hepatitis B virus infection in the United
States, 1976 to 1980. Am J Med 87: 5-10.
9.
Granovsky MO, Minkoff HL, Tess BH (1998) Hepatitis C
virus infection in the mothers and infants cohort study. Pediatrics 102:
355-359.
10.
Alter MJ (1995) Epidemiology of hepatitis C in the
west. Semin Liver Dis 15: 5-14.
11.
Jones DB (1989) Trouble on the border: International
health problems merge at the Rio Grande. Tex Med 85: 28-33.
12.
Hosmer DW, Lemeshow S (1989) Applied logistic
regression. New York John Wiley & Sons.
13.
Centers for Disease Control and Prevention (1996)
Prevention of hepatitis A through active or passive immunization:
Recommendations of the Advisory Committee on Immunization Practices (ACIP).
MMWR Morb Mortal Wkly Rep 45: 1-30.
14.
Redlinger T, O'Rourke K, VanDerslice J (1997) Hepatitis
A among schoolchildren in a US-Mexico border community. Am J Public Health 87:
1715-1717.
15.
Ruiz-Gomez J, Bustamante-Calvillo ME (1985) Hepatitis A
antibodies: prevalence and persistence in a group of Mexican children. Am J
Epidemiol 121: 116-119.
16.
Shapiro CN, Margolis HS (1993) Worldwide epidemiology
of hepatitis A virus infection. J Hepatol 18: 11-14
17.
Shapiro CN, Coleman PJ, McQuillan GM, Alter MJ,
Margolis HS (1992) Epidemiology of hepatitis A: Seroepidemiology and risk
groups in the USA. Vaccine 10: 59-62.
18.
Committee on Infectious Diseases American Academy of
Pediatrics (1996) Prevention of hepatitis A infections: Guidelines for use of
hepatitis A vaccine and immune globulin. Pediatrics 98: 1207-1215.
19.
Liu Z, Hou Z (2006). Hepatitis B virus (HBV) and
hepatitis C virus (HCV) dual infection. Int J Med Sci 3: 57-62.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Food and Nutrition-Current Research (ISSN:2638-1095)
- Advances in Nanomedicine and Nanotechnology Research (ISSN: 2688-5476)
- Journal of Veterinary and Marine Sciences (ISSN: 2689-7830)
- Journal of Biochemistry and Molecular Medicine (ISSN:2641-6948)
- Journal of Agriculture and Forest Meteorology Research (ISSN:2642-0449)
- Journal of Womens Health and Safety Research (ISSN:2577-1388)
- Journal of Genetics and Cell Biology (ISSN:2639-3360)


